 |
| Closeup image of the Brown-Roberts-Wells stereotactic system, the first device to incorporate the N-localizer that was invented by a third-year medical student, Russ Brown, MD, PhD, working with researchers in the Department of Radiology in 1978. The N-localizer forever changed the world of neurosurgery. Photo: Michael Mozdy. |
By Michael Mozdy
“You’re the guy who saved my wife’s life,” is a phrase few researchers expect to hear in their lifetimes. Yet it’s something Russ Brown, MD, PhD, a University of Utah School of Medicine graduate and inventor of the N-localizer, has had the pleasure of hearing. Since his days at the U when he invented the device, Brown has personally met a handful of people whose loved ones have had neurosurgery guided by the N-localizer. He marvels at how an elegant mathematical solution has led to life-saving neurosurgical interventions for more than a million patients.1
As a third year medical student at the U in 1978, Brown realized he preferred math and computers to direct patient care. “I needed to find a research elective,” he recalls, “or my fourth year of medical school would be filled with numerous clinical rotations that didn’t appeal to me.”
 |
| Jim Nelson, MD, who was Brown’s mentor. |
A colleague told him to visit Jim Nelson, MD, a radiologist who was doing interesting work two floors down in the basement of University Hospital. Nelson was a physician scientist who tirelessly pursued innovative solutions to medical problems; he, together with Jim Sorenson, PhD, and Bob Kruger, PhD, laid the foundation for what would become the Utah Center for Advanced Imaging Research (UCAIR).
“A big, tall, redheaded 3rd year medical student came down to my office one day,” reminisces Nelson. Brown was casting about for a research topic, and Nelson took note of his interests and strengths. Nelson had started out as a general surgeon and had scrubbed in on several stereotactic surgery cases, which were plagued by imprecision. “I explained to Russ the basics of stereotaxis,” recalls Nelson. “The guy’s got incredible brain power. He’d focus on a subject for three weeks and by the time he came back he knew more about it than most people.”
Brown launched himself into understanding the challenge. “After drawing on the board with me one day,” says Nelson, “he disappeared for about a month and then came back to my office and said, ‘I’ve worked out the solution, I know how to make it work.’” During the previous month, Brown came up with something that would change neurosurgery forever.
Stereotaxis and the Educated Guess
Doing any kind of surgical procedure on the brain is not easy. There’s the problem of the hard skull and squishy brain underneath, which make getting inside tricky and dangerous. More importantly, physicians need to know the exact point at which to operate since a few millimeters’ misstep in any direction could be disastrous.
Physicians in the early 1900s began brain surgery on animals (mainly rats) with the help of a frame rigidly fixed to the skull and a basic understanding of brain anatomy that came from centuries of dissections and illustrations. Their estimates of where to drill into the skull were based on common anatomical landmarks like the edge of the eye socket and the base of the cranium. The frame helped them aim their drill in what came to be called stereotactic surgery.
 |
| The Horsely-Clarke Apparatus, 1908, an early stereotactic device used for animals. Photo: Cyber Museum of Neurosurgery. |
By the 1940s, stereotactic frames had been adapted for human neurosurgery. Neurosurgeons could treat various disorders like Parkinson’s disease by destroying some tissue in a particular part of the brain. At this time, x-rays revealed some basic information about cranial anatomy, but no information about the underlying brain. Even with a stereotactic frame guiding surgery, precision boiled down to an educated guess. As a result, any stereotactic procedure was very dangerous; if the surgeon missed the intended target by even a few millimeters, the patient could end up in a vegetative state. By the late 1960s, the drug L-DOPA was introduced as a medical treatment for Parkinson’s disease and stereotactic surgery fell into disuse.
But stereotactic surgery was poised for a thrilling comeback in the mid-1970s with the invention of the computerized tomography (CT) scanner. Suddenly, neurologists had access to images of the brain with exquisite contrast. If there was a way to map the CT scan to the three dimensions of physical space around the patient’s head, then neurosurgeons could perform stereotactic surgery with much greater accuracy and safety.
Nothing a Little Triangulation and Linear Algebra Can’t Solve
Physician researchers were trying to tackle the problem of merging CT scans and stereotactic surgery when Brown met with Nelson about a research elective. After reading the published studies Nelson gave him, Brown began to get some ideas. “There was no mathematical sophistication,” Brown relates, “the problem wasn’t even articulated very well. There was no way to enforce a relationship between the scan image and the stereotactic frame.”
CT scans are a collection of two-dimensional x-ray images, each taken as a “slice.” CT slices may contain a point of interest for a physician, but translating that two-dimensional point to the three dimensions of a patient’s head in a stereotactic frame is not a trivial task. “It was necessary to transform (u, v) coordinates from the two-dimensional coordinate system of the CT image into (x, y, z) coordinates in the three-dimensional coordinate system of a stereotaxic frame,” Brown explains. But there was no consistent point of reference in the CT image or on the frame that could help to orient and connect the two.
Brown’s clear understanding of the problem, coupled with his knowledge of geometry and linear algebra, led him to an elegant solution that could be manufactured directly into a stereotactic frame. He realized that attaching a diagonal rod to the frame would produce an elliptical landmark in the CT image. As the CT scans moved progressively upward with respect to the diagonal rod, the ellipse that marked where the rod intersected the slice would move from one side of the CT image to the other. Better yet, he realized that placing the diagonal rod between two vertical rods to form an “N” would produce two circles that mark fixed beginning and end points for measuring the movement of the ellipse (see illustration).
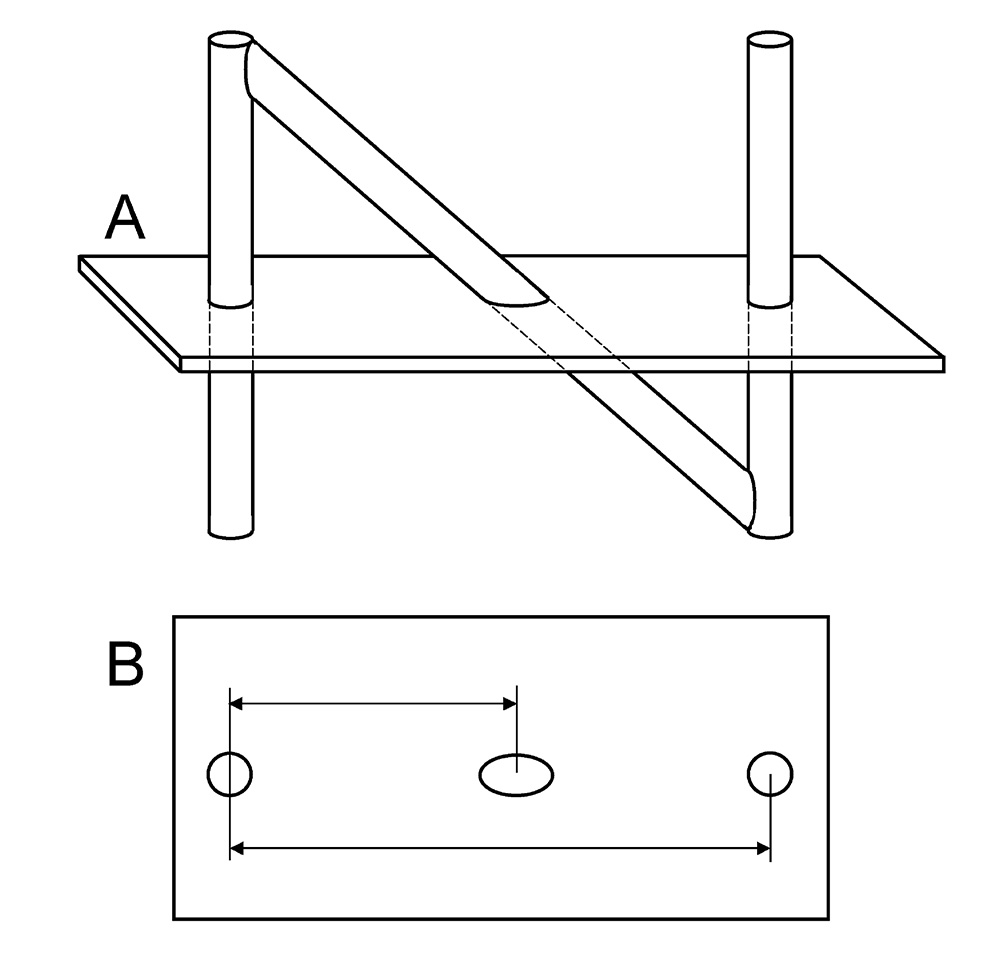 |
The concept behind the N-localizer: A) shows the N-shaped combination of rods and the intersection of these rods with the CT scan plane, and B) shows the resulting CT image. The circles and ellipse are produced by the intersections of the rods with the CT scan plane. As this plane moves upward with respect to the diagonal rod, the ellipse moves away from one circle and towards the other circle. Measurement of the distances between the circles and the ellipse provides information to orient the CT image to the stereotactic frame. Illustration first published in 2. |
The next challenge for Brown was that CT scanners have some mechanical imprecision, meaning that the plane of the CT scan slice could be oriented in any position relative to the frame. Brown needed to know exactly how the slice was oriented with respect to the frame, so he placed three N-localizers on the frame so they would encircle a patient’s head. This way, any CT slice contains three different points that intersect the N-localizers and thereby define the plane of the CT scan (see illustration).
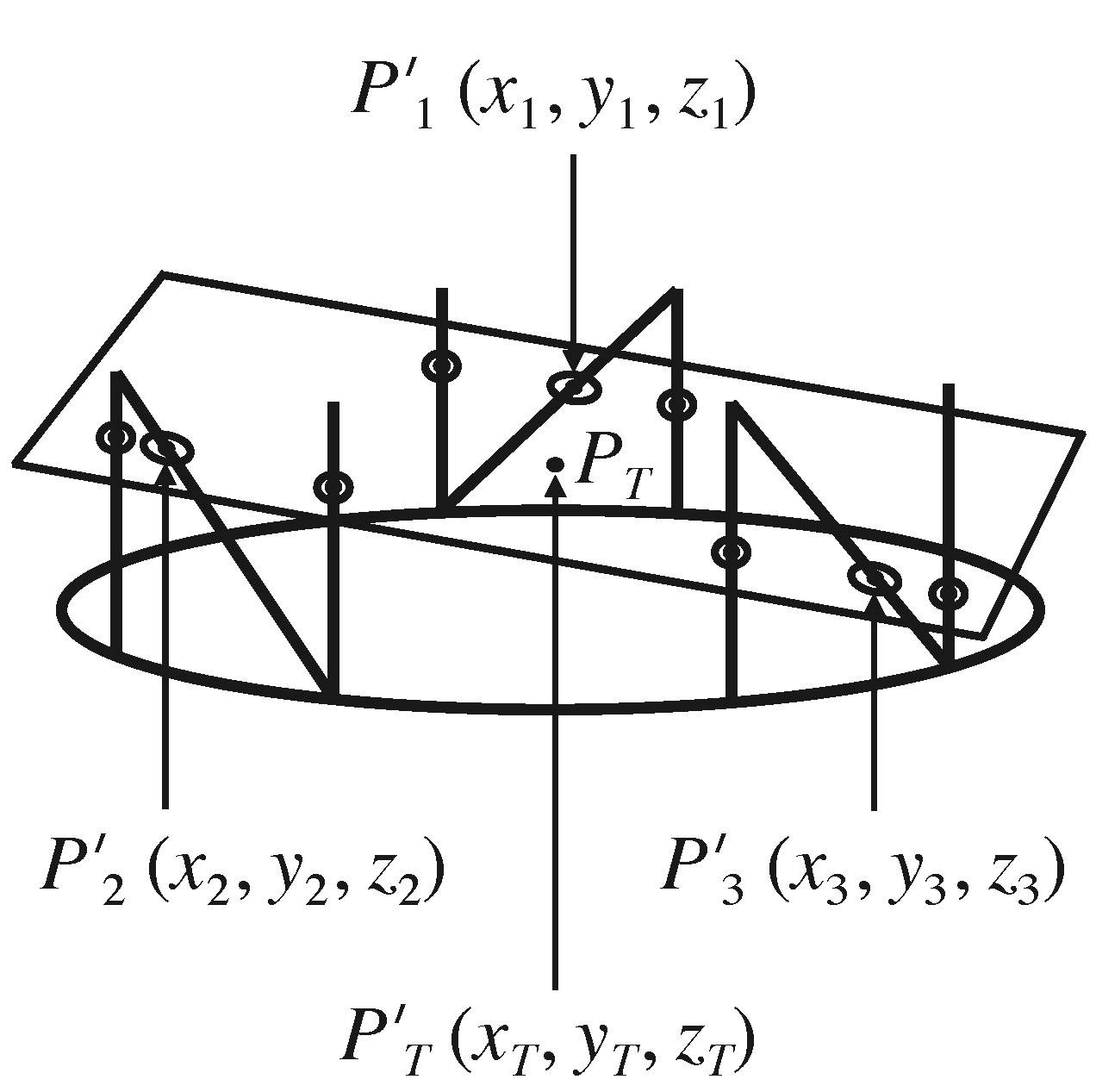 |
Three N-localizers precisely determine the orientation of the CT scan plane (the rectangle) relative to the base of the stereotactic frame (the oval). Brown used the intersection points Pʹ1, Pʹ2, and Pʹ3 of the diagonal rods to transform the target point PT from the two-dimensional coordinate system of the CT image into PʹT in the three-dimensional coordinate system of the stereotactic frame. Illustration first published in 3. |
Because three N-localizers provide Brown with the points of intersection and the plane of the CT scan, he is able to apply what is called a matrix transformation, a little bit of linear algebra that helps to convert two dimensional points into a three-dimensional coordinate system and vice versa. This gives him what the neurosurgeons need: an exact
(x, y, z) coordinate within the patient’s brain where they want to reach.
“The N-localizer made possible neuro-navigation”
From Concept to Widespread Neurosurgery
Brown knew he was onto something, and after showing his work to Nelson, he displayed a true researcher’s resourcefulness and set about creating his own prototype. He whipped up some engineering drawings and bought some Lucite sheets, rods, and spheres. “I’m a guy whose only manufacturing experience was limited to wood shop in 8th grade,” he laughs, “but in about two weeks I had built a prototype stereotactic frame that incorporated the N-localizer.”
 |
| Photo of Russ Brown, MD, PhD, as a medical student with his prototype stereotactic frame and N-localizers. |
The system had two parts: the N-localizers on a ring (indispensable for orienting CT scans), and an adjustable arc-based system used by neurosurgeons to directly access the point of interest within a patient’s brain. The particular genius of Brown’s system was that he wrote software that would help neurosurgeons quickly adjust the frame. Neurosurgeons would simply type the (u, v) coordinates from their CT scan point of interest into a handheld calculator, and Brown’s software (which he wrote using principles that he learned while working at the world’s first computer graphics company, Evans and Sutherland, in Salt Lake City) would return the four arc angles and a depth that the neurosurgeons would use to reach their target.
Brown began testing the device. Suspended inside the frame were some small spheres that served as targets. Using CT scans of the frame and spheres, Brown dialed the appropriate angles into the stereotactic frame and successfully targeted the spheres. The device was as accurate as Brown had hoped, achieving an average deviation from the target point of 2mm.
Nelson encouraged Brown to demonstrate the prototype for Ted Roberts, MD, the chief of Neurosurgery at the U of U. Roberts immediately saw its value and asked his colleague Peter Heilbrun, MD, to help test this tool in the operating room. The two were both pilots, and their time navigating the skies gave them insight into how important Brown’s invention was for navigating the brain. First, they needed to find someone who could manufacture a stereotactic frame built with N-localizers. They knew just who: Trent Wells, another pilot who flew P-51 Mustang fighter planes in World War II. Wells had spent the past 30 years building medical instruments, including other stereotactic frames that didn’t yet have the N-localizers for use with CT scanners.
 |
| Trent Wells (center) with other pilots, April 22, 1946. |
Wells was intrigued, and after some time discussing with Brown and Roberts, retreated to his workshop to engineer the manufactured model. With funding from Roberts and ongoing consultation with Brown on the design, Wells turned the idea into the Brown-Roberts-Wells stereotactic system, or BRW frame for short. This production frame was even more precise than the prototype, achieving an average deviation from the target point of just 1mm.
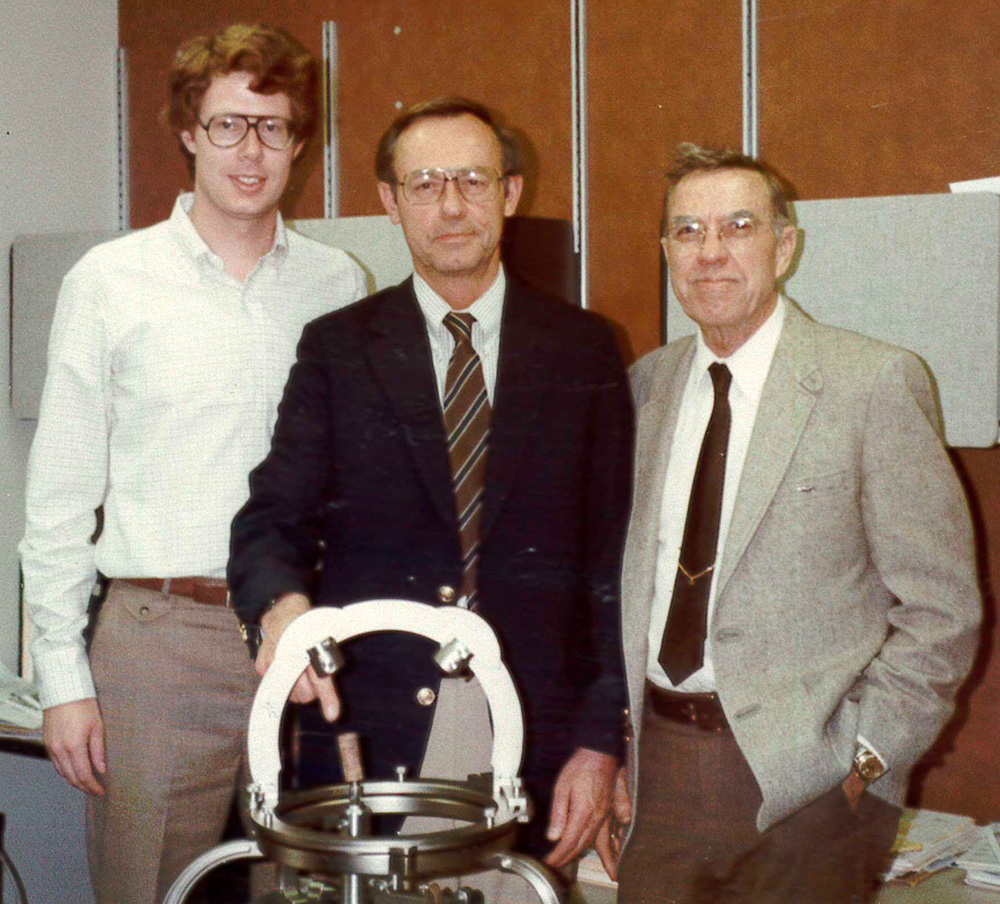 |
| Russ Brown, Ted Roberts, and Trent Wells posing with an early manufactured version of the Brown-Roberts-Wells stereotactic system. © University of Utah. |
Now it was up to practicing neurosurgeons to test the BRW frame and prove its usefulness. Roberts and Heilbrun were prepared to begin using it in Utah, although their patient base was relatively modest. They found an eager ally in early 1979 at the Richard Lende Winter Neurosurgery Conference, held at Snowbird Ski Resort in Utah. A promising young neurosurgeon from USC named Michael Apuzzo, MD, attended what he calls “the ski conference” put on by Roberts and the U of U Department of Neurosurgery. Apuzzo recalls, “I happened to see this contraption – a plastic frame for doing stereotactic neurosurgery – sitting on a table at the conference.” It was Brown’s prototype.
Apuzzo was friends with Roberts and Heilbrun, who introduced him to Wells and Brown and spoke with him about the device. Apuzzo, who was looking for a way to incorporate accurate CT scans into stereotactic neurosurgery, pledged his support and collaboration for testing it with the large volume of patients he saw at Los Angeles County General Hospital.
|
|
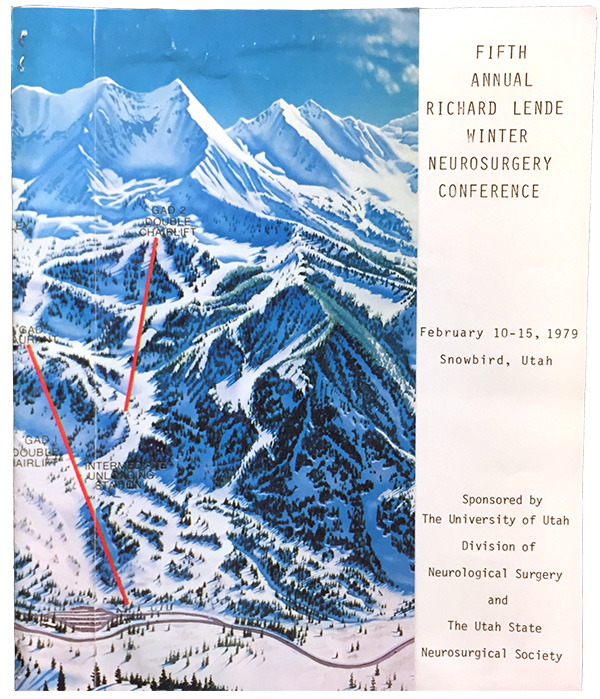
The original 1979 Richard Lende Winter Neurosurgery Conference program where Apuzzo first saw Brown’s prototype frame and pledged his support for testing the manufactured BRW frame introduced later that year. © University of Utah. |
The first neurosurgeon to use the BRW frame was Roberts at the U of U. Apuzzo soon followed with the very first production BRW frame (serial number 1) given to him by Wells. Apuzzo performed thousands of procedures and helped to prove the efficacy and accuracy of the system, publishing on his own and again in collaboration with Heilbrun. Wells gave a second BRW frame to David Thomas, MD, a neurosurgeon in London, who together with George du Boulay, MD, and Robert Anderson, MD, the chief of neuroradiology at the U of U, performed independent tests of the BRW.5
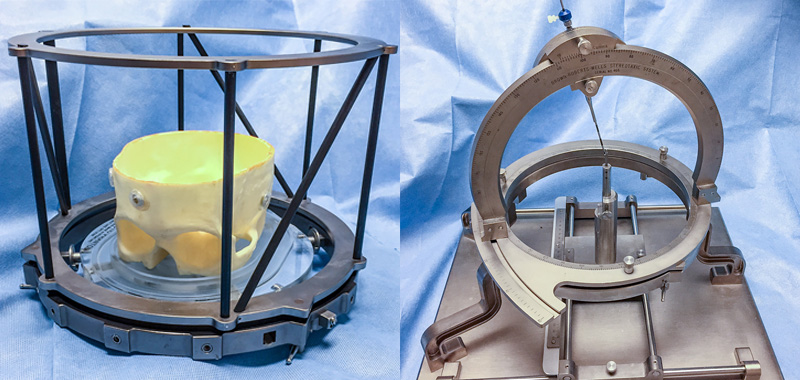 |
| The two interchangeable parts of the BRW frame: the N-localizer ring (left, shown surrounding a partial skull model) and the stereotactic arc-based surgical system (right). Each component fit onto the bottom ring (shown at bottom on left), which was secured to the patient’s head, allowing the patient to move in between scanning and the operating room while maintaining accuracy of the stereotactic system. |
“Russ [Brown] made an important contribution to patient care,” verifies Apuzzo, who is now recognized as one of the world’s most influential neurosurgeons and has dozens of honors and awards from around the world. “The University of Utah was so important to imagination at the time. Peter [Heilbrun] was a brilliant guy, Ted [Roberts] was great, and there were others like Anne Osborn, a neuroradiologist present at the first surgery using the BRW who also had an important book published – so many innovative elements.”
The illustration below shows how the BRW frame was used.
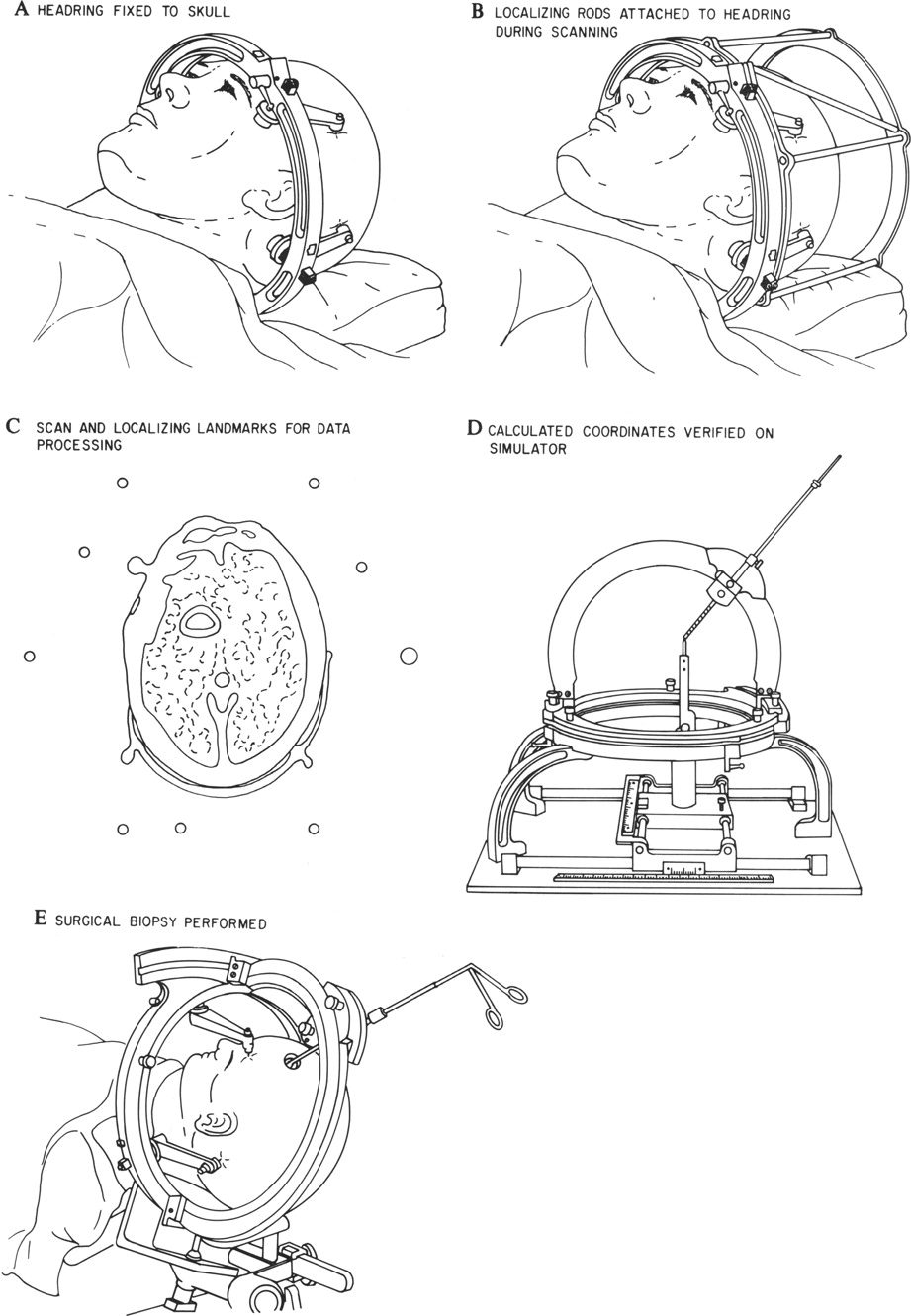 |
Use of the BRW stereotaxic guidance system. A: The head ring is fixed to the skull. B: The localizing rods (N-localizers) are attached to the head ring during CT scanning. C: A sample CT scan image from which the coordinates of nine localizing rods and of an intracranial target point are obtained for use in subsequent computation. D: Computed stereotactic frame settings are verified for correct trajectory and depth to target on the simulator. E: The arc guidance system is attached to the head ring, and the intracranial procedure is performed. Illustration and text first published in 4. |
“The N-localizer made possible neuro-navigation,” Brown asserts, and once that was possible, the applications were many. It has been used with CT, magnetic resonance (MR), and positron emission tomography (PET). Neurosurgeons have used it to guide tissue biopsies, evacuations, aspirations, and cultures; to guide functional neurosurgery, where various brain structures are destroyed; and to guide brachytherapy, where sealed radiation sources are placed inside or adjacent to a brain tumor in order to kill the tumor cells. And probably the most important application of the N-localizer is to guide stereotactic radiosurgery, where external x-rays or gamma rays are aimed at a brain tumor to kill the tumor cells. More than one million patients have been treated via stereotactic radiosurgery guided by the N-localizer.1
 |
| Russ Brown, MD, PhD. |
The N-localizer helped to usher in an era of more targeted and precise intracranial treatment.
After the BRW frame, six other frames were adapted to use the N-localizer system and, to the best of Brown’s knowledge, all of them use his mathematical transformations. Not too shabby for a third-year medical student looking for a research project in 1978!
The Department of Radiology and Imaging Sciences is proud to be a place where trainees and faculty with varied interests can find stimulating work with practical and far-reaching impacts. We’re proud of alumni like Russ Brown who apply themselves so completely and for alumni like Jim Nelson, Ted Roberts, and Peter Heilbrun, who have the ability to see trainees’ talents and mentor them towards success.
We look forward to sharing the stories from more alumni who have made a difference in the practice of medicine.
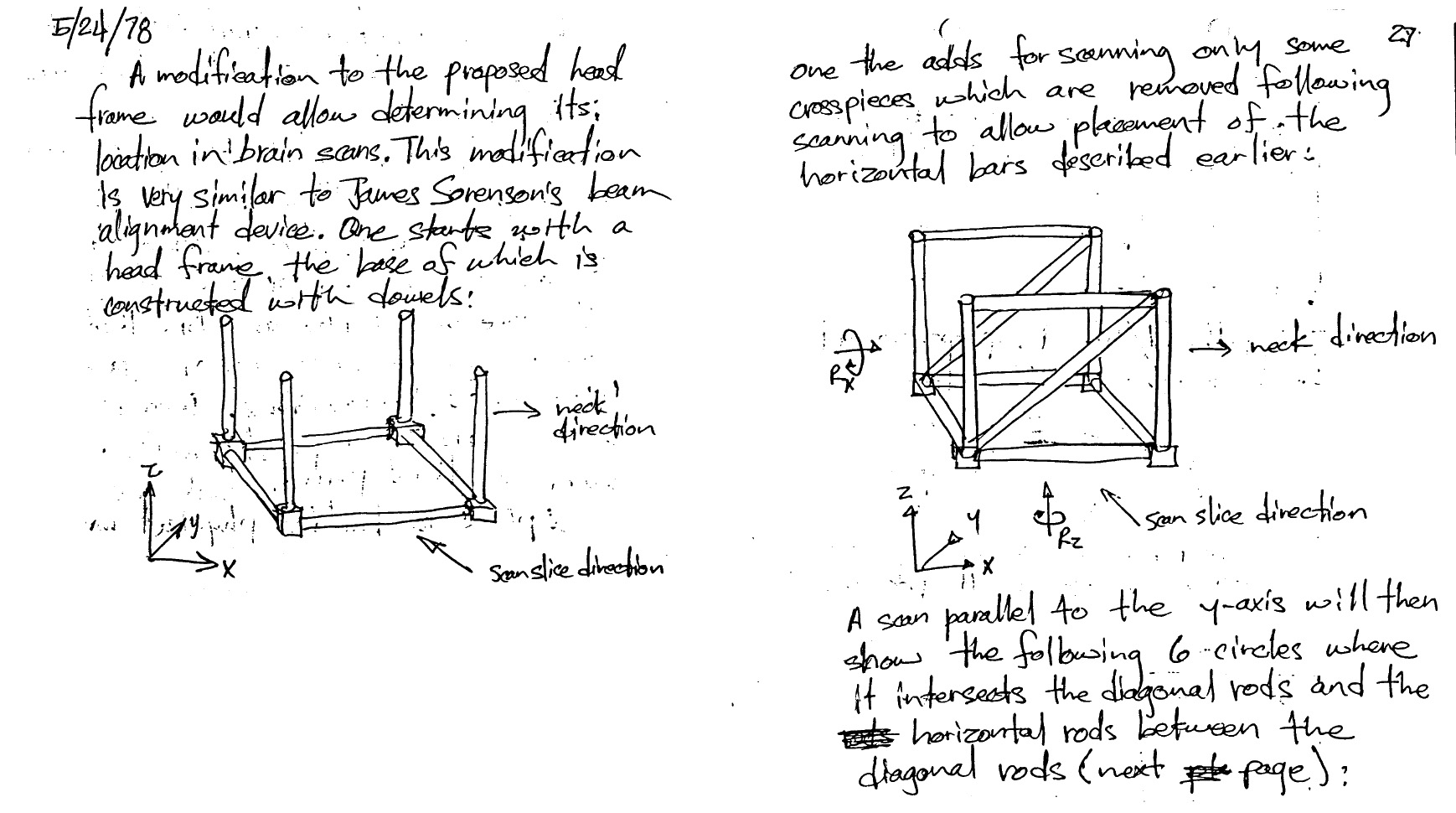
Pages from Russ Brown’s med school notebook (first published in appendix to 2):
1 Leksell D, Lunsford LD. The Origins and Birth of the Leksell Gamma Knife. Intracranial Stereotactic Radiosurgery, 2nd Edition. Lunsford LD, Sheehan JP (ed): Thieme Medical Publishers, Inc., New York; 2015, 1:1-10.
2 Brown RA, Nelson JA. The Invention and Early History of the N-Localizer for Stereotactic Neurosurgery. Cureus. 2016, 8(6): e642.
3 Brown RA. The Mathematics of Three N-Localizers Used Together for Stereotactic Neurosurgery. Cureus. 2015,7(10): e341.
4 Heilbrun MP, Roberts TS, Apuzzo ML, Wells TH Jr, Sabshin JK. Preliminary Experience with Brown-Roberts-Wells (BRW) Computerized Tomography Stereotaxic Guidance System. Journal of Neurosurgery. 1983, 59(2), 217-222.
5 Thomas DGT, Anderson RE, du Boulay GH. CT-Guided Stereotactic Neurosurgery: Experience in 24 Cases with a New Stereotactic System. Journal of Neurology, Neurosurgery, and Psychiatry. 1984, 47(1), 9-16.